It relates: {Savings, Investment, Population growth} -> Inputs{Labour, Capital stock, Technology} -> {Outputs}
We looked at two models
a) the Neo-classical: Assumes laws of diminishing returns apply to capital and thus production output. It also does not account for the effect of technological progress. The economy thus reaches a steady state(Point at which savings and required investments are equal- above this point,there is no more growth and even increase in savings would have no overall effect on growth.


b) the endogenous model:assumes absence of diminishing returns such that savings and productivity can thus grow exponentially.
With the move to the endogenous model, it is clear that the rate of growth depends on the type of capital that a country invests in. Human capital can generate long term sustained growth- this is because of its role in fostering innovation for technological progress, industry. This makes a good case for investment in health and education.
Health impacts income through 4 main mechanisms(Bloom D. et al 2003):
1. Labour productivity: less time lost off work if staff are healthy and they are thus often more productive.
2. Education: Increased attendance, increased ability to learn, healthy adults have more money to invest in child education. Also with an increased life expectancy, there is greater incentive to invest many yrs in education.
3. Savings & Investment: Longer prospective life increases incentive to save; Countries with fewer communicable diseases tend to be more 'attractive' to foreign investors; large health costs often force families to lose assets; Governments also tend to spend large amounts on health when it is poor- this money can be reallocated to industry if health is good.
4. Age distribution: This was already discussed here.
Also, there was a brief discussion on health inequalities and their influence on economic development. I thought this was an interesting image:
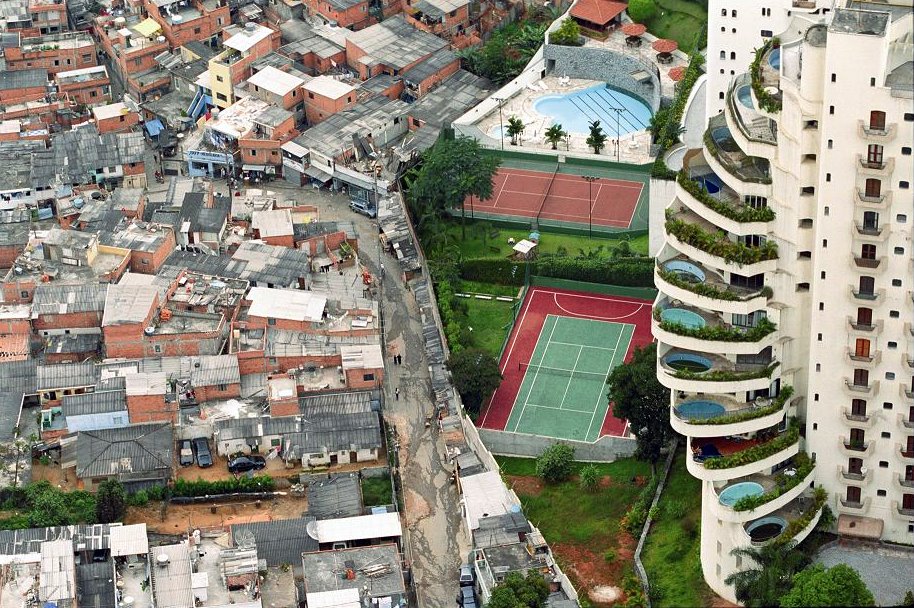 |
| http://www.sumit4all.com/life/the-india-of-today |
Sometimes the disparities are not very far away!
It was estimated that if a country reduces its health gap by 1%, there would be an annual increment in economic growth by 0.15%
26/04/13
Inequalities in health are a consequence of a variety of factors. In Uganda,according to the demographic Health Study(2001),women with higher education(secondary school and above) have fertility rate of 3.9 compared to those with lower education whose fertility rate was 7.3 - 7.8 children per woman. And research done by Lawson et al showed that smaller families are less likely to be poor and increase in family size was one of the factors that caused families to transit into poverty. These large family sizes also impact on health of the children. MFPED showed that reduction of one birth over 5 years reduced infant mortality risk by 30%
References:
Lawson, D., A. McKay, and J. Okidi. 2003. Poverty Persistence and Transitions in Uganda: A Combined Quantitative and Qualitative Analysis. CPRC Working Paper No. 38
MFPED. 2002. Infant Mortality in Uganda. Why the Non-improvement. Kampala: MFPED
26/04/13
Inequalities in health are a consequence of a variety of factors. In Uganda,according to the demographic Health Study(2001),women with higher education(secondary school and above) have fertility rate of 3.9 compared to those with lower education whose fertility rate was 7.3 - 7.8 children per woman. And research done by Lawson et al showed that smaller families are less likely to be poor and increase in family size was one of the factors that caused families to transit into poverty. These large family sizes also impact on health of the children. MFPED showed that reduction of one birth over 5 years reduced infant mortality risk by 30%
References:
Lawson, D., A. McKay, and J. Okidi. 2003. Poverty Persistence and Transitions in Uganda: A Combined Quantitative and Qualitative Analysis. CPRC Working Paper No. 38
MFPED. 2002. Infant Mortality in Uganda. Why the Non-improvement. Kampala: MFPED
No comments:
Post a Comment